Predictors of Lethality, Remodeling, and Aorta-Related Events in Different Types of Proximal Aortic Dissection Surgery
The aim of the study is to analyze predictors of lethality, false lumen thrombosis, enlargement of aortic diameter, and frequency of aorta-related events in the early and remote postoperative periods for various types of proximal aortic dissection surgery using the logistic regression method.
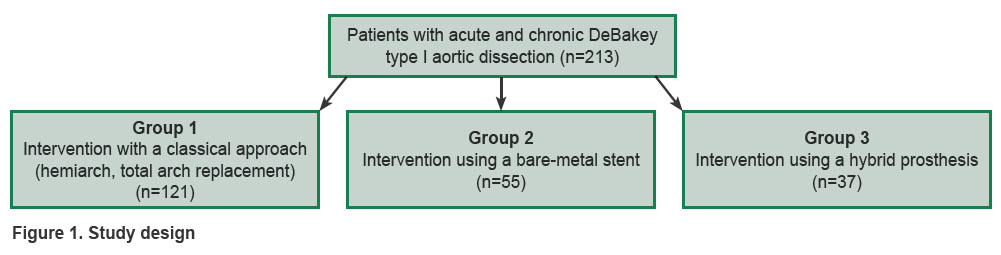
Materials and Methods. A retrospective observational comparison of the results of surgical treatment of 213 patients with the diagnosis of “DeBakey type I aortic dissection” has been carried out. The participants were divided into three groups: group 1 underwent classic aortic arch reconstruction using hemiarch technique or total reconstruction of the aortic arch with a multiple-branch prosthesis (n=121); group 2 was subjected to the hemiarch technique and implantation of bare-metal (uncoated) stents (n=55); in group 3, the “frozen elephant trunk” correction technique was used (n=37). The diagnosis of all patients included into the study was preoperatively confirmed by ultrasound and tomographic examination. Predictors of negative events have been identified by building the models of logistic regressions.
Results. The multivariate model of logistic regression has revealed multiplicative significant predictors of lethality: postoperative neurological complications increased the probability of lethality by 3.39 (1.24–9.18) times and presence of a patent false lumen by 4.17 (1.49–13.68) times.
Among the predictors of aorta-related events, the most important were connective tissue diseases (the probability increased by 6.68 (2.98–15.62) times), presence of partial thrombosis of the false lumen (the probability of event development increased by 2.39 (1.07–5.44) times), and aortic valve repair (the probability aorta-event occurrence increased by 2.84 (1.13–7.17) times).
Hybrid prosthesis implantation appeared to be the most significant predictor of false lumen thrombosis increasing its probability by 4.19 (1.90–9.44) times among aortic repair methods, while a bare-metal stent implantation in contrast reduced the likelihood of false lumen thrombosis by 0.17 (0.03–0.62) times. Eventually, the type of repair had not any significant impact on the aorta-related events and lethality in the long-term period.
Introduction
Despite many factors aggravating essentially the condition of patients with proximal aortic dissection, the results of surgical treatment of this cohort of patients are gradually improving owing to timely diagnosis and the surgical intervention performed. Nevertheless, the rate of hospital lethality remains within the range of 10–30% [1–6].
Presently, concurrently with classic (traditional) intervention, i.e. repair of the ascending aorta and the arch using hemiarch or total arch replacement techniques, implantation of supplementary devices such as bare-metal stents or stent grafts into the descending aorta has become technically feasible [7]. However, the effectiveness of these extended interventions on aorta has been insufficiently studied so far.
Having analyzed the results of the standard approach to the aorta reconstruction, Suzuki et al. showed in their study [8] that actuarial freedom from reoperations was 96.9, 83.2, 64.2, and 58.3% after 1, 5, 10, and 12 years, respectively. Regression analysis of Cox proportional hazards allowed the authors to identify the following independent predictors of late repeated operation: young age, malperfusion, proximal fenestration in the ascending aorta, descending aorta diameter, F/T>1 index (ratio of false and true lumen diameter in the region of the descending aorta), and the Marfan syndrome.
Presence of the patent false lumen is one of the main predictors of postoperative aorta remodeling, and therefore the risk of repeated interventions — it is the very postulate that became the basis of the surgical strategy of treating aortic dissection [9]. Despite the desire for maximum readaptation of the dissected aortic walls, the effectiveness of various surgical techniques in achieving this goal differs considerably. Thus, the “elephant trunk” operation, suggested by H.G. Borst in 1983, did not contribute to turning off aneurysm and/or false lumen from the bloodstream [10, 11]. The advent of new prostheses and technologies moved surgeons along the path of greater radicalism in performing primary reconstructions of proximal aortic dissections. However, advantages of these interventions are still unobvious. For example, the effectiveness of Djumbodis Dissection System implantation (a bare-metal stent) has repeatedly been called into question. According to the literature data, stenting of the true lumen with a bare-metal stent results in thrombosis of a false lumen only in 68% of cases in acute and in 18–20% in chronic dissection, which cannot compete with actually 100% thrombosis over 5 years using the technique of “frozen elephant trunk” [7, 12–14].
Although the results of surgical treatment of proximal aortic dissections are gradually improving with time, operation lethality remains steady within 18–25% [5]. Taking into consideration anatomical variability of aortic dissections and a wide choice of surgical correction techniques, the analysis of aorta-related event predictors and the resulting repeated surgical interventions is of great interest [15].
The aim of the study is to analyze predictors of lethality, false lumen thrombosis, enlargement of aortic diameter, and frequency of aorta-related events in the early and remote postoperative periods for a variety of proximal aortic dissection repair using the logistic regression method.
Materials and Methods
A retrospective observational study has been performed. The results of surgical treatment of 213 patients with the diagnosis of “DeBakey type 1 aortic dissection” were compared. In all patients, dissection involved ascending aorta, aortic arch, and descending thoracic aorta. Patients operated on in the clinics of Meshalkin National Medical Research Center (Novosibirsk, Russia), Cardiology Research Institute of Tomsk National Research Medical Center of the Russian Academy of Sciences (Russia), and University Hospital of Amiens (France) from 2001 to 2017 were included in the study.
Participants were divided into three groups:in group 1, standard surgical approaches were applied (hemiarch technique or total reconstruction of the aortic arch (n=121)); group 2 was subjected to the hemiarch technique and implantation of bare-metal stents (n=55); in group 3, the “frozen elephant trunk” technique was used (n=37) (Figure 1).
|
Figure 1. Study design |
The diagnosis of all patients included into the study was preoperatively confirmed by ultrasound and tomographic examination. False lumen thrombosis was assessed over the whole lumen length irrespective of the anatomical zone. Absence of false lumen contrast was considered as total thrombosis, no signs of false lumen thrombosing denoted complete patency defined by the contrast-enhanced MSCT examination. Any events related to aorta (ruptures, dissections) as well as interventions on aorta and aortic valve over the entire follow-up period were referred to aorta-related events.
Statistical data processing. Sampling distribution of continuous indicators was checked for normality of distribution using the Shapiro–Wilk test. The terms of observation appeared abnormal, therefore, comparison was carried out with the help of non-parametric Mann–Whitney U-test with the correction of multiple comparison error using the Benjamini–Hochberg test. To assess the value of difference in the groups, a pseudomedian of value differences and standardized mean difference (SMD) were calculated. The continuous indicators were presented as median, 25th and 75th percentiles (Me [Q1; Q3]), mean and standard deviation (M±SD). Binary indicators were described as the number of events and frequency with the construction of a 95% confidence interval using the Wilson formula (n/%, 95% CI).
Negative event predictors were identified building the models of logistic regressions. By means of single-factor models, separate predictors associated with a target event were determined. Covariate population with the achieved level of significance of p<0.3 in single-factor models was employed to build models of multifactor logistic regression optimally complying with the Akaike information criterion using forward and backward stepwise selection method. All models of the forward and backward step coincided. For the multifactor model of the logistic regression, the best classification threshold in terms of sensitivity/specificity ratio was detected by the ROC analysis methods, the contingency table was built to calculate prognostic indicators: sensitivity, specificity, frequency of method occurrence, actual frequency of occurrences. Goodness of fit for prognostic frequencies of the calibrated model and actual frequencies of negative events was studied by means of the Hosmer–Lemeshow test.
Statistical hypotheses were checked at the critical level of significance of p=0.05, i.e. differences were considered statistically significant at p<0.05.
All statistical calculations were performed in R-Studio program (version 2022.07.2+576 Spotted Wakerobin, USA) using R language (version 4.1.3, Austria).
Results
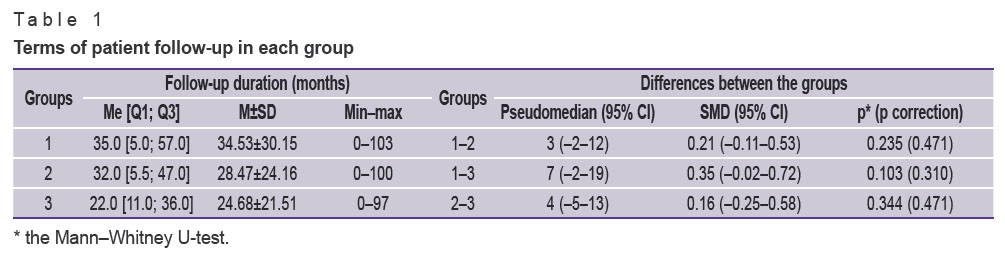
The patients were followed up in-person or remotely. A mean period of observation was calculated separately for each group (Table 1).
|
Table 1. Terms of patient follow-up in each group |
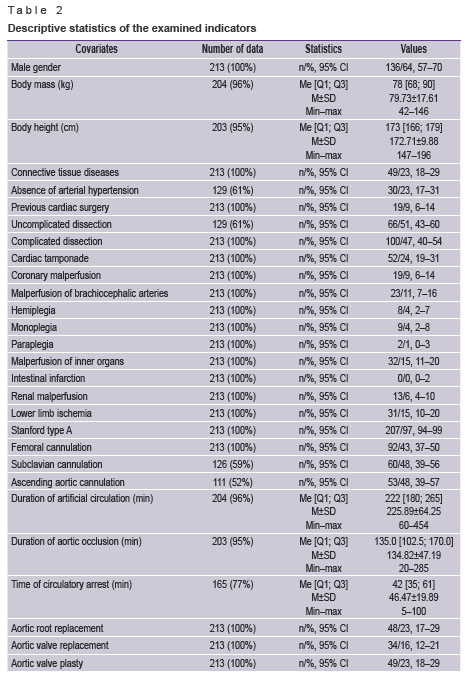
The descriptive statistics of the examined covariates is presented in Table 2.
|
Table 2. Descriptive statistics of the examined indicators |
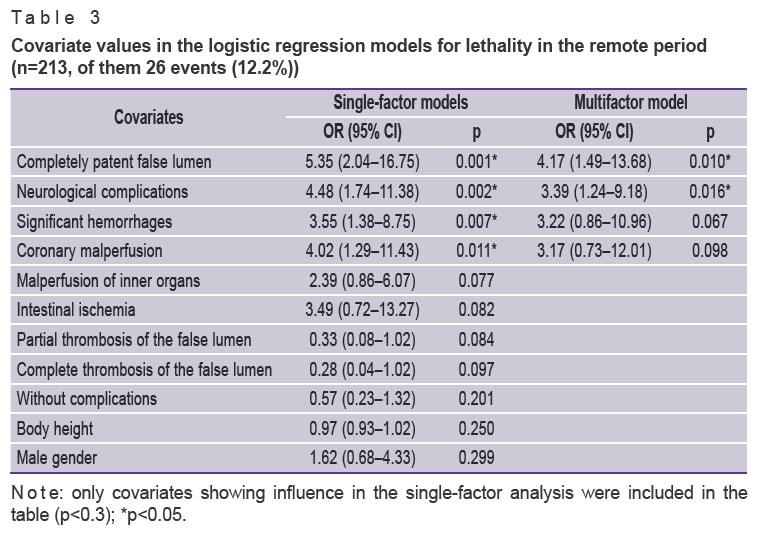
The logistic regression method for single-factor and multifactor models was used for identification of lethality predictors in the remote period (Table 3). Building single-factor models of logistic regression, separate significant predictors of lethality were found. For example, coronary malperfusion and significant hemorrhages increased the probability by 3.17 and 3.22 times, respectively, however, when these covariates were included in the multifactor model, their significance reduced. Building of the multifactor model of logistic regression has demonstrated that neurological complications in the postoperative period increased the probability of lethality by 3.39 (1.24–9.18) times, and presence of the completely patent lumen by 4.17 (1.49–13.68) times.
|
Table 3. Covariate values in the logistic regression models for lethality in the remote period (n=213, of them 26 events (12.2%)) |
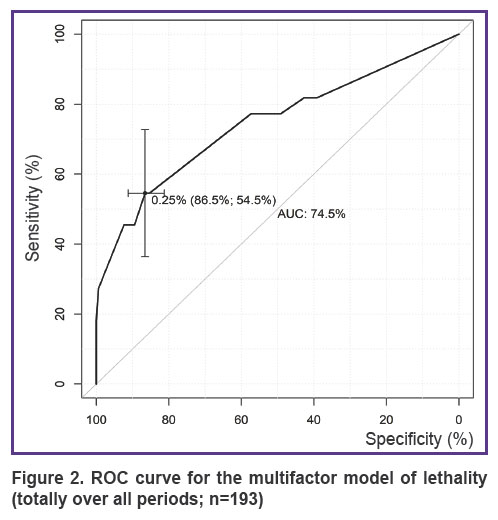
For the threshold lethality value in the remote period equal to 24.8%, the best indicators of sensitivity (54.5%) and specificity (86.5%) in terms of the balance (Figure 2) were determined for the multifactor model using the ROC analysis.
|
Figure 2. ROC curve for the multifactor model of lethality (totally over all periods; n=193) |
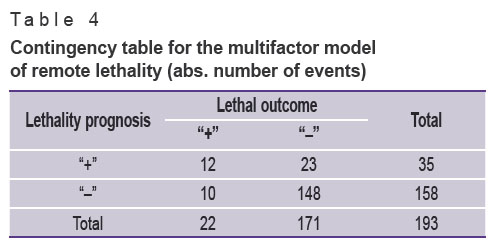
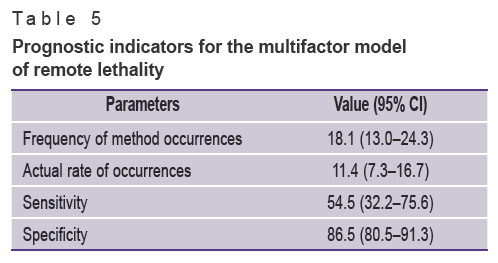
In order to investigate prognostic properties of the multifactor model for remote lethality, a contingency table (Table 4) has been created and prognostic indicators have been calculated (Table 5). The total number of patients in the multifactor model was 193, which was 20 patients fewer than in the general sample due to the missed data in the covariates.
|
Table 4. Contingency table for the multifactor model of remote lethality (abs. number of events) |
|
Table 5. Prognostic indicators for the multifactor model of remote lethality |
The level of significance obtained for the Hosmer–Lemeshow test (p=0.245) demonstrated goodness of fit for prognostic frequencies of the calibrated model and the actual frequency of remote lethality. The complex metrics (AUC=74.5) showed a satisfactory quality of the model classification (see Figure 2).
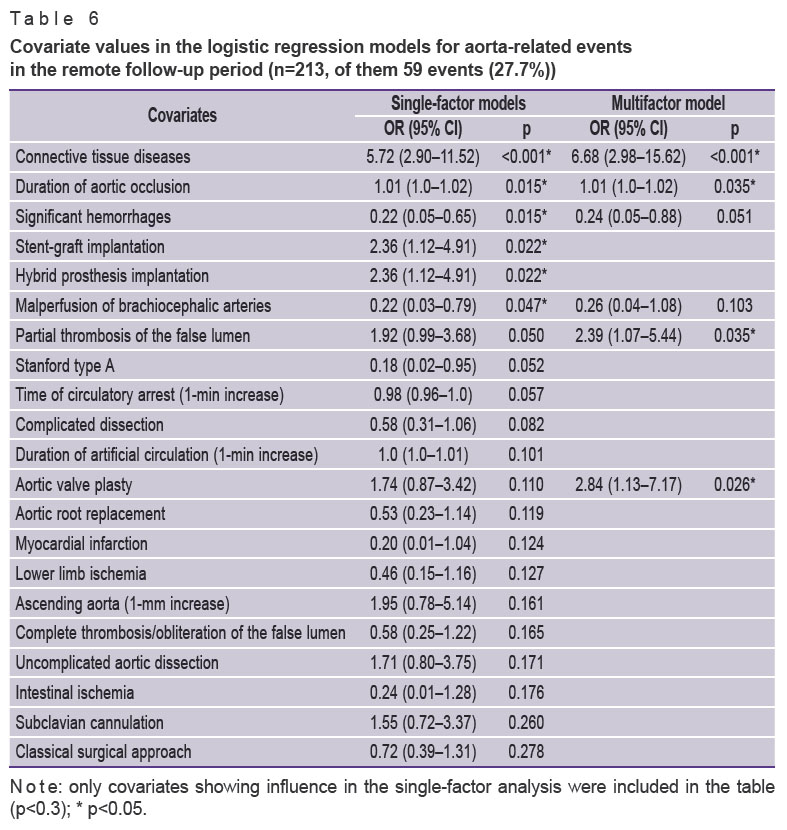
The logistic regression method for a single-factor and multifactor model was applied to determine predictors of aorta-related events (Table 6). Several factors had a strong influence on the occurrence of aorta-related events in the remote period. Diseases of the connective tissue increased the probability of the event by 6.68 (2.98–15.62) times, partial thrombosis of the false lumen by 2.39 (1.07–5.44) times. Aortic valve repair increased the probability of aorta-related events by 2.84 (1.13–7.17) times, which may speak of the necessity of thorough valve revision and its more frequent replacement. It should be also noted that significant bleedings in the postoperative period reduced the likelihood of aorta-related events in the remote period (0.24 (0.05–0.88) at р=0.051).
|
Table 6. Covariate values in the logistic regression models for aorta-related events in the remote follow-up period (n=213, of them 59 events (27.7%)) |
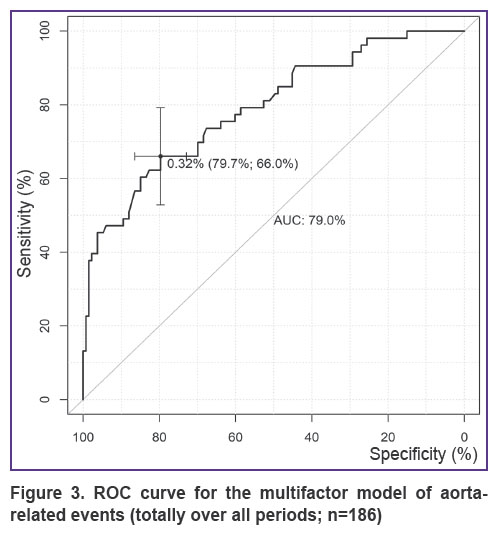
For the threshold value of the probability of aorta-related events (totally over all periods), equal to 32.4%, the best indicators of sensitivity (66%) and specificity (79.7%) (Figure 3) were determined for the multifactor model using the ROC analysis.
|
Figure 3. ROC curve for the multifactor model of aorta-related events (totally over all periods; n=186) |
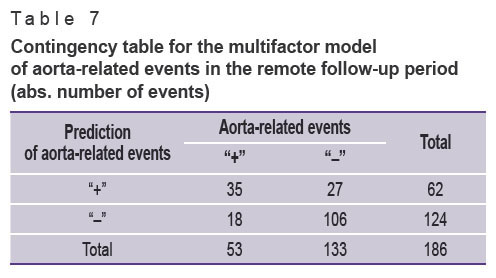
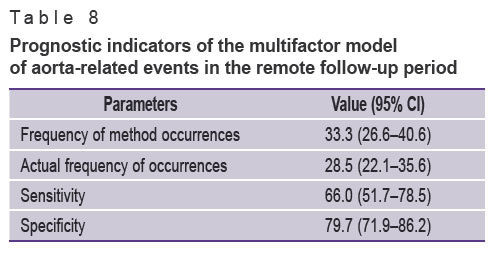
In order to investigate prognostic properties of the multifactor model for aorta-related events, a contingency table (Table 7) has been created and prognostic indicators have been calculated (Table 8). The total number of patients in the multifactor model was 186, being 27 patients fewer than in the general sample due to the missed data in the covariates.
|
Table 7. Contingency table for the multifactor model of aorta-related events in the remote follow-up period (abs. number of events) |
|
Table 8. Prognostic indicators of the multifactor model of aorta-related events in the remote follow-up period |
The level of significance obtained for the Hosmer–Lemeshow (p=0.670) test demonstrated goodness of fit for prognostic frequencies of the calibrated model and the actual frequency of aorta-related events. The complex metrics (AUC=79.0%) showed a satisfactory quality of the model classification (see Figure 3).
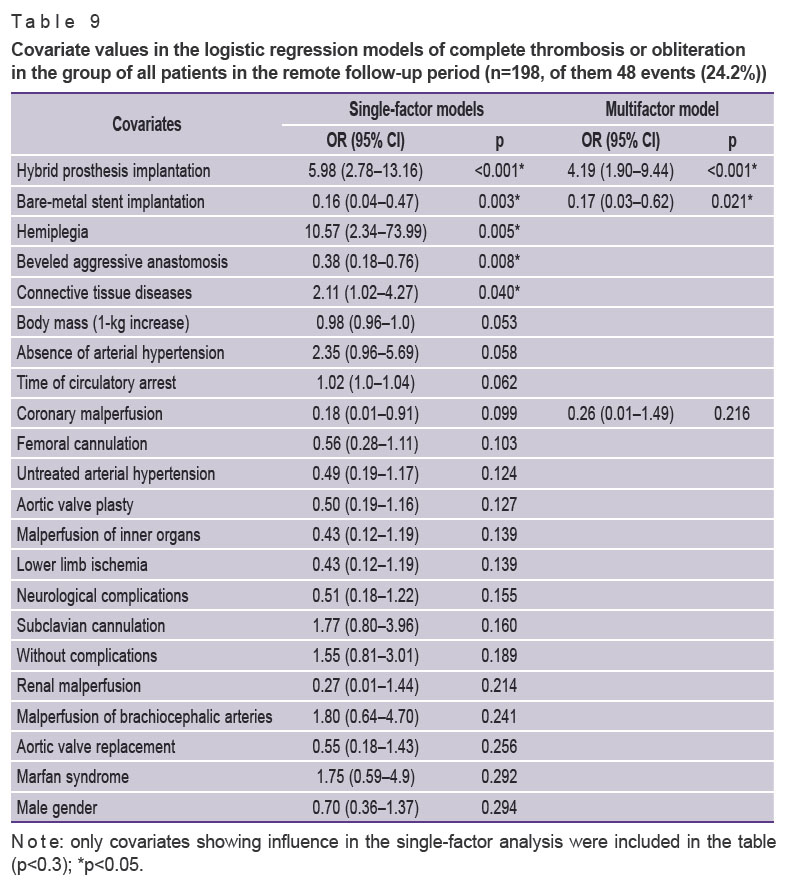
There has been analyzed the effect of factors on the occurrence of thrombosis and complete obliteration of the aortic false lumen in 198 patients (Table 9), which was 15 patients fewer than in the general sample due to the missing data in the target indicator.
|
Table 9. Covariate values in the logistic regression models of complete thrombosis or obliteration in the group of all patients in the remote follow-up period (n=198, of them 48 events (24.2%)) |
As one can see from Table 9, implantation of a hybrid aortic prosthesis (group 3) was the strongest predictor of false lumen thrombosis in the remote period increasing its probability by 4.19 (1.90–9.44) times. Implantation of a bare-metal stent (group 2), on the contrary, reduced false lumen thrombosis by 0.17 (0.03–0.62) times.
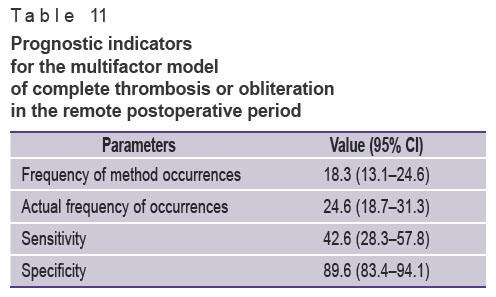
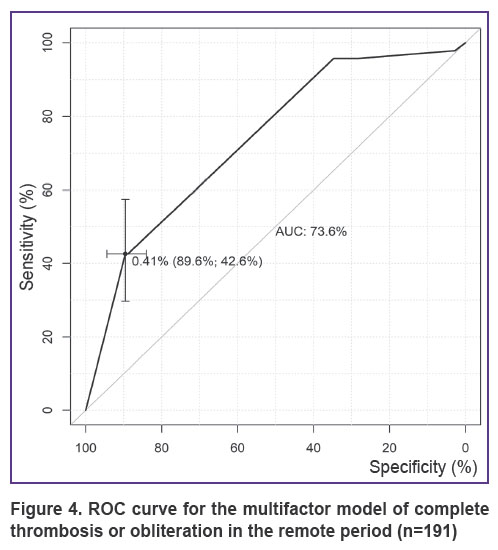
For the 40.9% threshold value of the probability of complete thrombosis/obliteration in the postoperative period, the best indicators of sensitivity (42.6%) and specificity (89.6%) (Figure 4) were determined for the multifactor model by means of the ROC analysis. Using the threshold value obtained, complete thrombosis/obliteration of the aortic false lumen was predicted.
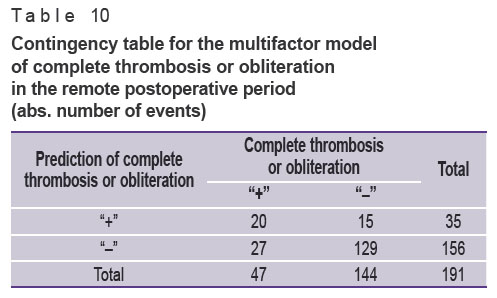
In order to investigate prognostic properties of the multifactor model for complete thrombosis or obliteration in the remote postoperative period, a contingency table (Table 10) has been created and prognostic indicators have been calculated (Table 11). The total number of patients in the multifactor model was 191, being 22 patients fewer than in the general sample due to the missed data in the covariates.
|
Table 10. Contingency table for the multifactor model of complete thrombosis or obliteration in the remote postoperative period (abs. number of events) |
|
Table 11. Prognostic indicators for the multifactor model of complete thrombosis or obliteration in the remote postoperative period |
The level of significance of the Hosmer–Lemeshow (p=0.007) has shown that the prognostic values of the calibrated model do not fit the actual frequencies of complete thrombosis or obliteration in the remote postoperative period. The complex metrics (AUC=73.6) demonstrated a satisfactory quality of the model classification (see Figure 4).
|
Figure 4. ROC curve for the multifactor model of complete thrombosis or obliteration in the remote period (n=191) |
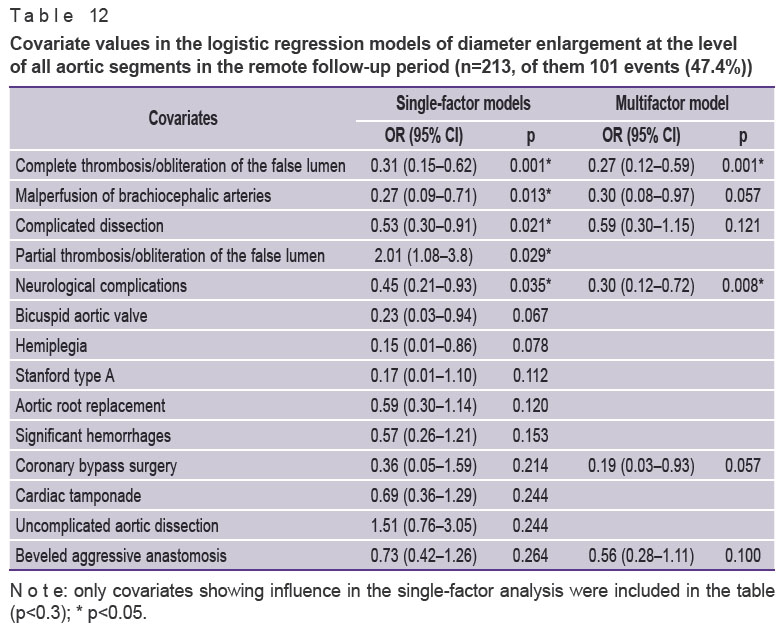
To identify predictors of enlargement of the descending aortic arch diameter, the four segments of aorta (aortic arch and three descending thoracic segments) were considered as a single section. To define predictors of enlargement of the abdominal aortic arch diameter, the two aortic segments (abdominal and infrarenal) were also considered as a single section. A single-factor and then multifactor complete and optimal analysis of predictors have been carried out (Table 12).
|
Table 12. Covariate values in the logistic regression models of diameter enlargement at the level of all aortic segments in the remote follow-up period (n=213, of them 101 events (47.4%)) |
The single-factor analysis has revealed several statistically significant predictors of aorta enlargement. When building a multifactor model, complete thrombosis or obliteration of the false lumen turned out to be the strongest predictor reducing the probability of widening thoracoabdominal aorta. This predictor decreased the event probability by 0.27 (0.12–0.59) times (p=0.001). Another unexpected strong predictor reducing the probability of aorta enlargement was the development of neurological complications in the postoperative period (0.30 (0.12–0.72) at p=0.008).
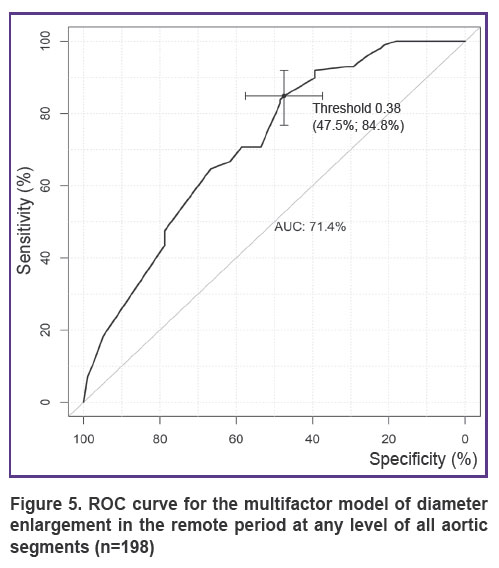
Using the ROC analysis, the best indicators of sensitivity (84.8%) and specificity (47.5%) (Figure 5) have been determined for the multifactor model at the 38.1% threshold value for the diameter enlargement probability at the level of all aortic segments. Using the obtained threshold value, enlargement of aortic diameter at any level has been predicted.
|
Figure 5. ROC curve for the multifactor model of diameter enlargement in the remote period at any level of all aortic segments (n=198) |
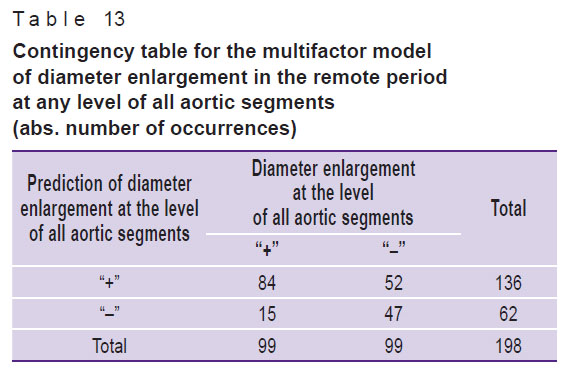
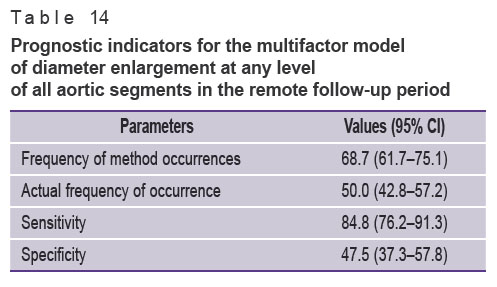
To investigate the prognostic properties of the multifactor model of diameter enlargement at any level of all aortic segments, a contingency table (Table 13) was created and prognostic indicators were calculated (Table 14). The total number of patients in the multifactor model was 198, being 15 patients fewer than in the general sample due to the missing data in covariates.
|
Table 13. Contingency table for the multifactor model of diameter enlargement in the remote period at any level of all aortic segments (abs. number of occurrences) |
|
Table 14. Prognostic indicators for the multifactor model of diameter enlargement at any level of all aortic segments in the remote follow-up period |
The level of significance obtained for the Hosmer–Lemeshow test (p=0.147) demonstrated goodness of fit for prognostic frequencies of the calibrated model and the actual frequency of diameter enlargement at the level of all segments. The complex metrics (AUC=71.4%) shows a satisfactory quality of the model classification (see Figure 5).
Discussion
Over several recent decades, disputes on the selection of the surgical intervention volume in treating type I aortic dissection were focused on whether primary reconstruction of the proximal dissection should be done within the limits of the ascending segment and aortic arch. Evidently, hospital survival in primary intervention does not ensure the development of aorta-related events requiring surgical reinterventions since the majority of patients, who survived the primary correction of aortic dissection, have persisting dissected part of the aorta and/or distal fenestration [16].
It has been shown in some studies [4, 17] that an extended volume of the primary reconstruction of proximal dissection in the form of aortic arch repair reduces frequency of late aortic complications and improves long-term survival. At the same time, there are reports showing that complete replacement of the aortic arch does not eliminate the necessity of repeated operations or reduces remote lethality. For example, Larsen et al. [18], having analyzed the remote results of 334 patients undergone operations for complete aortic arch replacement and 907 hemiarch reconstructions, did not find any differences in a general 5-year survival (73.1 vs. 69.4%; р=0.83). In our study, the analysis of the intervention type effect on the lethality did not detect strong relations between these indicators in the remote follow-up period.
Predictors of lethality in the remote period (within 5 years) were identified using the logistic regression method. Presence of neurological complications in the postoperative period has been found to increase the probability of lethality by 3.39 (1.24–9.18) times, while completely patent lumen increased it by 4.17 (1.49–13.68). Our results agree with the data presented by Olsson et al. [19], who reported a strong impact of neurological complications on the survival of patients with aortic dissection.
Reoperations on aorta in patient survived an acute period of dissection do not happen rarely. In the study performed by Kirsch et al. [20], actuarial freedom from redo operations was 60.8±6.8% after 10 years, in the work of Fattouch et al. — 81.3% within 10 years [21]. Kim et al. [22] have shown that the rate of the reoperations did not depend on the type of aortic arch reconstruction: 5-year freedom from repeated operations was 88% in the group of the total aortic arch replacement and 92.8% in the group with the hemiarch reconstruction.
The analysis of predictors of aorta-related events after a primary reconstruction has shown that connective tissue diseases increased the probability of event occurrence by 6.68 (2.98–15.62) times. The results obtained by us were in line with the previously published data on the effect of connective tissue dysplasia on the frequency of aorta-related events in the remote period [21, 23]. Fattouch et al. [21] have detected statistically significant difference between patients with the Marfan syndrome and without it in the extent of the false lumen obliteration. According to the Cox regression analysis performed by the authors, presence of the Marfan syndrome was a predictor of a late surgical reintervention on the descending aorta.
One more important factor of the ongoing pathological remodeling of aorta and development of unfavorable outcome in the remote period is the presence of a patent false lumen [24–26]. It has been shown in some works [27, 28] that patency of the false lumen was preserved in 26.5–39.4% of cases after the first stage of reconstruction. In the process of our investigation, the presence of partial thrombosis of the false lumen was found to increase the probability of the event by 2.39 (1.07–5.44) times.
Thrombosis of the false lumen is a critically important factor influencing the lethality rate in the remote follow-up period. In the study of Tsai et al. [29], partial thrombosis of the false lumen was a key predictor of mortality (the relative risk of 2.69; 95% CI: 1.45–4.98; р=0.002). According to our results, implantation of a hybrid prosthesis was a strong predictor of complete false lumen thrombosis increasing the probability of the event by 4.19 (1.90–9.44) times, whereas implantation of a bare-metal stent affects negatively the occurrence of thrombosis reducing its probability by 0.17 (0.03–0.62) times. This agreed with the data on a positive effect of a hybrid prosthesis implantation on remodeling of the aortic lumen [17], however, the fact of the negative influence of the bare-metal stent implantation on the remodeling has been revealed for the first time.
Since it is the presence of the patent false lumen that determines the risk of subsequent aorta dilation, one of the main criteria influencing the decision to perform intervention on aorta is enlargement of its diameter (5 cm or more) or the rate of its widening (according to the data of the sequential studies, more than 5 mm over 6 months of observation). For example, Fattori et al. [24] and Halstead et al. [30] have found that the annual rate of aorta growth was maximum in the descending segment and considerably higher in patients with an open false lumen; the mean growth rate was 1 mm/year. The initial sizes of aorta were also of significance for the outcomes of surgical aortic dissection reconstruction. It has been noted by Fattouch et al. [21] that the initial diameter of the descending aorta greater than 4.5 cm is a predictor of the late repeated intervention (hazard ratio (HR) of 5.8; 95% CI: 3.5–22.5; p=0.002).
In our study, the presence of complete thrombosis or obliteration of the false lumen appeared to be the strongest predictor diminishing the probability of widening of all aortic segments and reducing the probability of the event by 0.27 (0.12–0.59) times (p=0.001). Another unexpected strong predictor determining the probability of aortic enlargement was the development of neurological complications in the postoperative period increasing the probability of the event by 0.30 (0.12–0.72) times (p=0.008). It may be explained by the fact that the majority of neurological events in aortic dissection were connected with a more complex and lengthy intervention on the aortic arch, which in its turn increased the risk of neurological complications and the probability of thrombosis or obliteration of the false lumen. The analysis of the data for the thoracic aorta has shown that thrombosis or obliteration of the false lumen had also a significant influence on the reduction of aorta-related events in the remote period by 0.11 (0.03–0.28) times (p<0.001).
Limitations of the study. All models calculated by us have a satisfactory quality of predicting the events of lethality, aorta-related events, false lumen thrombosis, and enlargement of aortic diameter. However, other unaccounted factors may influence the emergence of these events. For example, multifocal atherosclerosis, cardiac rhythm disorder, ischemic heart disease, oncological diseases may affect the remote lethality indicators. Therefore, further investigation of the nonlinear relations of covariates and their intersections is quite necessary to make prognostic models more exact.
Conclusion
Our retrospective observational comparative study of the effectiveness of different types of proximal aortic reconstruction and the effect of various factors on the results has proved the negative influence of a bare-metal stent implantation on the process of postoperative aortic remodeling. At the same time, the type of intervention has no effect on the rate of aorta-related events and lethality in the remote follow-up period.
Study funding. The study was carried out within the framework of project No.22-15-20005 (Agreement No.22-15-20005 of March 22, 2022 with the Russian Science Foundation, Agreement No.R-12 of April 6, 2022 with the Ministry of Science and Innovation Policy of the Novosibirsk Region).
Conflicts of interest. The authors have no conflicts of interest to declare.
References
- Fann J.I., Smith J.A., Miller D.C., Mitchell R.S., Moore K.A., Grunkemeier G., Stinson E.B., Oyer P.E., Reitz B.A., Shumway N.E. Surgical management of aortic dissection during a 30-year period. Circulation 1995; 92(9 Suppl): II113–II121, https://doi.org/10.1161/01.cir.92.9.113.
- Kawahito K., Adachi H., Yamaguchi A., Ino T. Early and late surgical outcomes of acute type A aortic dissection in patients aged 75 years and older. Ann Thorac Surg 2000; 70(5): 1455–1459, https://doi.org/10.1016/s0003-4975(00)01934-2.
- Sinatra R., Melina G., Pulitani I., Fiorani B., Ruvolo G., Marino B. Emergency operation for acute type A aortic dissection: neurologic complications and early mortality. Ann Thorac Surg 2001; 71(1): 33–38, https://doi.org/10.1016/s0003-4975(00)01824-5.
- Kazui T., Yamashita K., Washiyama N., Terada H., Bashar A.H., Suzuki T., Ohkura K. Impact of an aggressive surgical approach on surgical outcome in type A aortic dissection. Ann Thorac Surg 2002; 74(5): S1844–S1863, https://doi.org/10.1016/s0003-4975(02)04155-3.
- Evangelista A., Isselbacher E.M., Bossone E., Gleason T.G., Eusanio M.D., Sechtem U., Ehrlich M.P., Trimarchi S., Braverman A.C., Myrmel T., Harris K.M., Hutchinson S., O’Gara P., Suzuki T., Nienaber C.A., Eagle K.A.; IRAD Investigators. Insights from the International Registry of Acute Aortic Dissection: a 20-year experience of collaborative clinical research. Circulation 2018; 137(17): 1846–1860, https://doi.org/10.1161/circulationaha.117.031264.
- Khvan D.S., Zhulkov M.O., Sirota D.A., Fomichev A.V., Chernyavskiy A.M. Aortic root repair in acute aortic dissection type A. Kardiologiya i serdechno-sosudistaya khirurgiya 2021; 14(1): 66–70, https://doi.org/10.17116/kardio20211401166.
- Sirota D.A., Khvan D.S., Lyashenko M.M., Alsov S.A., Zhulkov M.O., Chernyavsky A.M. Use of uncoated metal stents in surgery of aortic dissection. Angiologiia i sosudistaia khirurgiia 2018; 24(4): 110–116.
- Suzuki T., Asai T., Kinoshita T. Predictors for late reoperation after surgical repair of acute type A aortic dissection. Ann Thorac Surg 2018; 106(1): 63–69, https://doi.org/10.1016/j.athoracsur.2018.01.071.
- Uchida N., Katayama A., Tamura K., Sutoh M., Kuraoka M., Ishihara H. Frozen elephant trunk technique and partial remodeling for acute type A aortic dissection. Eur J Cardiothorac Surg 2011; 40(5): 1066–1071, https://doi.org/10.1016/j.ejcts.2011.02.074.
- Borst H.G., Walterbusch G., Schaps D. Extensive aortic replacement using “elephant trunk” prosthesis. Thorac Cardiovasc Surg 1983; 31(1): 37–40, https://doi.org/10.1055/s-2007-1020290.
- Greenberg R.K., Lu Q., Roselli E.E., Svensson L.G., Moon M.C., Hernandez A.V., Dowdall J., Cury M., Francis C., Pfaff K., Clair D.G., Ouriel K., Lytle B.W. Contemporary analysis of descending thoracic and thoracoabdominal aneurysm repair: a comparison of endovascular and open techniques. Circulation 2008; 118(8): 808–817, https://doi.org/10.1161/circulationaha.108.769695.
- Tsagakis K., Jakob H. Which frozen elephant trunk offers the optimal solution? Reflections from Essen Group. Semin Thorac Cardiovasc Surg 2019; 31(4): 679–685, https://doi.org/10.1053/j.semtcvs.2019.05.038.
- Messé S.R., Bavaria J.E., Mullen M., Cheung A.T., Davis R., Augoustides J.G., Gutsche J., Woo E.Y., Szeto W.Y., Pochettino A., Woo Y.J., Kasner S.E., McGarvey M. Neurologic outcomes from high risk descending thoracic and thoracoabdominal aortic operations in the era of endovascular repair. Neurocrit Care 2008; 9(3): 344–351, https://doi.org/10.1007/s12028-008-9104-9.
- Czerny M., Stöhr S., Aymard T., Sodeck G.H., Ehrlich M., Dziodzio T., Juraszek A., Carrel T. Effect on false-lumen status of a combined vascular and endovascular approach for the treatment of acute type A aortic dissection. Eur J Cardiothorac Surg 2012; 41(2): 409–413, https://doi.org/10.1016/j.ejcts.2011.05.063.
- Acheampong D.O., Paul P., Boateng P., Leitman I.M. Predictors and outcomes of cardiac events following thoracic endovascular aortic repair in descending thoracic aortic aneurysm and dissection. Aorta (Stamford) 2020; 8(1): 6–13, https://doi.org/10.1055/s-0040-1701606.
- Zierer A., Voeller R.K., Hill K.E., Kouchoukos N.T., Damiano R.J. Jr., Moon M.R. Aortic enlargement and late reoperation after repair of acute type A aortic dissection. Ann Thorac Surg 2007; 84(2): 479–487, https://doi.org/10.1016/j.athoracsur.2007.03.084.
- Sun L., Qi R., Zhu J., Liu Y., Zheng J. Total arch replacement combined with stented elephant trunk implantation: a new “standard” therapy for type a dissection involving repair of the aortic arch? Circulation 2011; 123(9): 971–978, https://doi.org/10.1161/circulationaha.110.015081.
- Larsen M., Trimarchi S., Patel H.J., Di Eusanio M., Greason K.L., Peterson M.D., Fattori R., Hutchison S., Desai N.D., Korach A., Montgomery D.G., Isselbacher E.M., Nienaber C.A., Eagle K.A., Bartnes K., Myrmel T. Extended versus limited arch replacement in acute type A aortic dissection. Eur J Cardiothorac Surg 2017; 52(6): 1104–1110, https://doi.org/10.1093/ejcts/ezx214.
- Olsson C., Hillebrant C.G., Liska J., Lockowandt U., Eriksson P., Franco-Cereceda A. Mortality and reoperations in survivors operated on for acute type A aortic dissection and implications for catheter-based or hybrid interventions. J Vasc Surg 2013; 58(2): 333–339.e1, https://doi.org/10.1016/j.jvs.2012.12.078.
- Kirsch M., Soustelle C., Houël R., Hillion M.L., Loisance D. Risk factor analysis for proximal and distal reoperations after surgery for acute type A aortic dissection. J Thorac Cardiovasc Surg 2002; 123(2): 318–325, https://doi.org/10.1067/mtc.2002.119702.
- Fattouch K., Sampognaro R., Navarra E., Caruso M., Pisano C., Coppola G., Speziale G., Ruvolo G. Long-term results after repair of type a acute aortic dissection according to false lumen patency. Ann Thorac Surg 2009; 88(4): 1244–1250, https://doi.org/10.1016/j.athoracsur.2009.06.055.
- Kim J.B., Chung C.H., Moon D.H., Ha G.J., Lee T.Y., Jung S.H., Choo S.J., Lee J.W. Total arch repair versus hemiarch repair in the management of acute DeBakey type I aortic dissection. Eur J Cardiothorac Surg 2011; 40(4): 881–889, https://doi.org/10.1016/j.ejcts.2010.12.035.
- Charchyan E.R., Abugov S.A., Khachatryan Z.R., Puretsky M.V., Khovrin V.V., Skvortsov A.A., Belov Yu.V. Postoperative care in patients with DeBakey type I aortic dissection: criteria of aortic remodeling and risk factors of disease progression. Khirurgiya. Zhurnal imeni N.I. Pirogova 2019; 5: 6–17, https://doi.org/10.17116/hirurgia20190516.
- Fattori R., Bacchi-Reggiani L., Bertaccini P., Napoli G., Fusco F., Longo M., Pierangeli A., Gavelli G. Evolution of aortic dissection after surgical repair. Am J Cardiol 2000; 86(8): 868–872, https://doi.org/10.1016/s0002-9149(00)01108-5.
- Rylski B., Milewski R.K., Bavaria J.E., Vallabhajosyula P., Moser W., Szeto W.Y., Desai N.D. Long-term results of aggressive hemiarch replacement in 534 patients with type A aortic dissection. J Thorac Cardiovasc Surg 2014; 148(6): 2981–2985, https://doi.org/10.1016/j.jtcvs.2014.05.093.
- Rylski B., Hahn N., Beyersdorf F., Kondov S., Wolkewitz M., Blanke P., Plonek T., Czerny M., Siepe M. Fate of the dissected aortic arch after ascending replacement in type A aortic dissection. Eur J Cardiothorac Surg 2017; 51(6): 1127–1134, https://doi.org/10.1093/ejcts/ezx062.
- Song S.W., Chang B.C., Cho B.K., Yi G., Youn Y.N., Lee S., Yoo K.J. Effects of partial thrombosis on distal aorta after repair of acute DeBakey type I aortic dissection. J Thorac Cardiovasc Surg 2010; 139(4): 841–847.e1, https://doi.org/10.1016/j.jtcvs.2009.12.007.
- Kirsch M., Legras A., Bruzzi M., Louis N. Fate of the distal aorta after surgical repair of acute DeBakey type I aortic dissection: a review. Arch Cardiovasc Dis 2011; 104(2): 125–130, https://doi.org/10.1016/j.acvd.2010.11.009.
- Tsai T.T., Evangelista A., Nienaber C.A., Myrmel T., Meinhardt G., Cooper J.V., Smith D.E., Suzuki T., Fattori R., Llovet A., Froehlich J., Hutchison S., Distante A., Sundt T., Beckman J., Januzzi J.L. Jr., Isselbacher E.M., Eagle K.A.; International Registry of Acute Aortic Dissection. Partial thrombosis of the false lumen in patients with acute type B aortic dissection. N Engl J Med 2007; 357(4): 349–359, https://doi.org/10.1056/nejmoa063232.
- Halstead J.C., Meier M., Etz C., Spielvogel D., Bodian C., Wurm M., Shahani R., Griepp R.B. The fate of the distal aorta after repair of acute type A aortic dissection. J Thorac Cardiovasc Surg 2007; 133(1): 127–135.e1, https://doi.org/10.1016/j.jtcvs.2006.07.043.








